10 AKI facts
Keep track of your kidney data with PKB
AKI used to be called ‘Acute Renal Failure (or ARF)’. AKI is simpler in some ways but there is no real injury, in a trauma sense.
We will now go through 10 facts about AKI.
1. Definition of AKI
AKI is a rapid reduction in kidney function – resulting in failure to (1) maintain the balance of water and chemicals, and (2) remove waste from the body.
AKI usually occurs over hours or days, and usually will require admission to hospital.
The normal job of the kidneys is to be the bodys’ dustmen and keep the levels of chemicals stable, and remove waste from the body. So when they do not work properly, you can become quite unwell, quite quickly.
AKI affects both of the kidneys, and is different from Chronic Kidney Disease (CKD) which has different causes, and occurs over months or years.
The primary problem is not usually the kidneys themselves. They are usually reacting to an underlying current serious condition, such as dehydration and infection (sepsis) after an operation – usually both. Therefore the patient’s medical condition will be dominated by the underlying disease (cause).

For many people, AKI (if it causes ATN, see below) lasts about 10-14 days but can be 2 days or 3 months. If the patient is still in AKI at 3 months, we normally assume CKD has started.
2. Why is AKI important?
- It is very common – 1 in 5 people admitted to hospital as an emergency have AKI
- AKI will double the patient’s average length of stay, and increase the readmission rate
- 90% of cases are ‘pre-renal’ (see later) and due to dehydration and sepsis
- Around 65% of AKI starts in the community, before the patient comes to hospital. But 35% are acquired in hospital, especially after surgery and some x-rays (angiograms, CTs etc)
- 30% are due to prescribed drugs
- 15 million people in the UK have diabetes, which puts them at greater risk of AKI
- The annual cost of AKI-related inpatient care in England is estimated at £1 billion, around 1% of the NHS budget.
Ok, so that’s the reason why it’s important. But ..
3. What are the causes of AKI?
The causes of acute kidney injury can be divided into prerenal, renal and post-renal. These phrases mean problems with the blood supply to the kidneys (pre), the kidneys themselves (renal), and the urine drainage pipes or bladder (post).
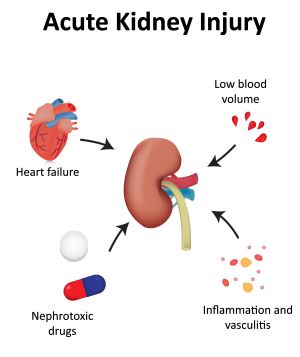
Pre-renal
- Dehydration and infection (sepsis) is the commonest cause. Other causes include:
- Bleeding (haemorrhage)
- Cardiac failure
- Low blood pressure
- Liver failure
- Blockages to the (renal) arteries to the kidneys (renal artery stenosis).
Renal
- Tubulo-interstitial disease (TID)
- Acute Tubular Necrosis (ATN). This is the commonest TI cause. It is usually secondary to prolonged hypoperfusion (largely all the prerenal causes). In ATN, the kidney is pre-programmed (for reasons we don’t understand) to ‘close down’ (blood goes to it and from it, but it is not filtered) for 10-14 days, and then it ‘opens up’ and starts doing its normal job again. Dialysis may be required during this period
- Drugs toxic to the kidneys – e.g. NSAIDs, ACEi/ARBs, antibiotics (such as aminoglycosides like gentamicin), or chemotherapy (such as cisplatin) and the dye that is injected for CTs and other x-rays (contrast nephropathy)
- Autoimmune diseases (all rare), such as:
- Glomerulonephritis (GN) (inflammation of tiny filtering units; in the cortex, see above diagram)
- Vasculitis (inflammation of small to medium sized blood vessels)
- Acute tubulointerstitial nephritis (TIN) (inflammation of tubes between the filtering units; in the medulla, see above diagram)
- Other: rhabdomyolysis, multiple myeloma, or haemolytic-uraemic syndrome (HUS; very rare)
Post-renal
- In men, it is usually due to enlargement of the prostate gland (benign (BPH) or malignant)
- In women, pelvic cancer is commonest cause
- Bladder cancer is another cause and can affect men and women.
Note. Renal stones are not a common cause of AKI, but can do – usually if you have one kidney.
4. What are the symptoms of AKI?
- Passing less urine (pee) than usual. However often the rate of urine production is normal (or even increased)
- Very concentrated urine, or urine looking yellow/brown/red in colour
- Loss of appetite, feeling sick (nausea) or vomiting
- Feeling tired and short of breath
- Feeling confused, anxious and restless, or sleepy
- Swelling of your legs, around eyes, and other body parts.
Note. There may be no symptoms and it is picked up on a routine blood test.
5. Medical assessment of someone with AKI
This involves the doctor asking you questions – especially related to your current condition (and surgery if you have had it) and what tablets you are on. This is followed by a careful examination, focussing on the amount of fluid in your body and your tummy. The blood pressure is very important.
Urine output
AKI is not usually determined by how much urine you make, as you can have quite severe AKI with normal (or even increased) urine output. Complete anuria (no urine output) is rare but always very serious. It has only three causes: ‘vascular catastrophe’ (complete disruption of kidney arteries; pre-renal), acute severe glomerulonephritis (renal) or complete urine blockage (post-renal).
6. What are the investigations for AKI?
- A urine dipstick helps to identify a potential underlying cause. Blood and protein suggest an autoimmune ‘renal cause’
- Blood tests should include:
- A special blood test called a ‘blood gas’ (taken from an artery at the wrist) if useful as it gives the doctor an idea of how unwell you are, and they will get the results back immediately
- A chest x-ray
- An ultrasound scan of the kidneys, ureters and bladder is required in more severe cases; especially if there is no response to initial treatment, to check you have two kidneys and look for post-renal (obstructive) causes
- Very rarely a kidney biopsy (removal of a piece of kidney) is required.
There is more about the investigations for AKI here on CKDEx.
7. What are the stages of AKI?
These are defined by the measurement of something called creatinine in the blood; the higher the creatinine, the worse the kidney function.
- AKI Stage 1: Serum creatinine 1.5–1.9 times baseline
- AKI Stage 2: Serum creatinine 2.0–2.9 times baseline
- AKI Stage 3: Serum creatinine ≥ 3.0 times baseline.
Stage 1 is the mildest (best) form, and Stage 3 the most severe (worst) form.
Distinguishing AKI and CKD
Most patients with AKI look unwell, may have hyperkalaemia (potassium > 6.0 mmol/L), and are either already admitted for something else or need admission and rapid review.
Patients with Chronic (i.e. long term) Kidney Disease (CKD) usually look well, and may have other complications of CKD (e.g. anaemia, low calcium, high PTH etc).
Patients can have both, i.e. AKI on the background of CKD (‘AKI-on-CKD’).
8. What is the treatment for AKI?
Acute kidney injury is a medical emergency, and treatment should be instigated ASAP. The treatment is determined by the cause, e.g:
- Pre-renal – intravenous fluids and antibiotics
- Renal – stop drugs, and treatment of rare causes with strong drugs to suppress the immune system
- Post-renal – unblock the bladder with a urinary catheter; or other procedures and operations
If this does not work, temporary dialysis may be required. The renal (kidney) team will be called to carry out this treatment, with transfer to their ward. A small number of more unwell patients will need intensive care.
Drug rationalisation
This is a very important part of treatment. Medications can both affect and be affected by the kidneys, so its important that medications are reviewed in cases of AKI.
Drugs to be potentially stopped (or dose reduced)
- ACEi and ARBs
- SGLT2 inhibitors
- Diuretics (if patient is dehydrated)
- NSAIDs
- Aminoglycoside antibiotics
- Potassium-sparing diuretics (due to risk of a high blood potassium (hyperkalaemia))
- Metformin (risk of lactic acidosis)
- Low-molecular weight heparin
- Opioids – e.g. morphine or codeine.
Note. Some of these drugs (especially the first three) will need to be restarted by the patient’s GP when they are better.
9. What is the prognosis (outlook) for AKI?
The outlook is largely dependent on the outlook of the underlying condition. The mortality is high. Overall it is over 10% (double the ‘normal’ mortality for a medical admission); 30% if transferred to a renal ward and 50% if dialysis is required there.
If the patient is on ICU (and on ventilator) the mortality is higher again (70%).
The kidney function usually returns to the baseline level. This usually happens in 10-14 days, and for most people by three weeks. A small number take upto 3 months.
However you may be at risk of repeat AKI which can lead to CKD. A small number patients end up needing permanent dialysis as their kidney function does not improve.
10. How can you prevention from occurring, especially in the community?
Answer. Sick Day Cards.
The primary aim is prevention of AKI through education of patients (making them aware of their higher AKI risk), regular medicines management reviews and ‘sick day guidance’.
Sick Day Cards should be given to vulnerable patients (especially the elderly, with on man drugs, and CKD).
These ask the patient to stop a range of drugs – including Metformin, ACE/ARB, SGLT2is, NSAIDs and diuretics – for a few days if they are feeling unwell (especially septic, e.g. fever, gastroenteritis, UTI). They also need to be encouraged to drink more when they are unwell (especially if septic).
These drugs usually need to be restarted 48 or more hours later, when better, and eating and drinking normally. Discuss that with your GP.
Summary
We have described 10 AKI facts – including its definition, causes, investigation, treatment and prevention. Most people will make a full recovery.
Other resources
There is more information on Acute Kidney Injury (AKI) (Acute Renal Failure) written by the renal team at UHCW, Coventry.
This is good doctors review article.
This is another simpler doctor’s article.
And this is a good video especially related to the classification and investigation of AKI: https://www.simpleosce.com/interpretation/disease-specific/acute-kidney-injury.php.
This article was reviewed by Rachael Lee, AKI Advanced Nurse Practitioner, UHCW Coventry.
Last Reviewed on 5 April 2024