In a recent paper by Gandhi, 2023, a patient with COVAN (COVID-19-associated nephropathy) was described.
The term ‘COVAN’ has been used to describe collapsing focal segmental glomerulosclerosis (FSGS) in people who have been infected with SARS-CoV-2.
This helps differentiate it from the majority of cases of acute kidney injury in COVID-19 patients, which are typically caused by acute tubular injury.
The treatment of COVAN is centered on supportive measures including dietary sodium restriction, optimisation of hyperlipidaemia and hypertension, RAAS blockade, and diuresis for oedema.
There is limited evidence to support the use of steroids in COVAN. However, the mechanism of podocytopathy is similar to that in HIVAN (HIV-associated nephropathy); with both being more likely in people with an APOL1 gene mutation.
Based on previous experience, treatment of HIVAN with steroids is beneficial and safe in selected patients. Hence the approach was tried on this patient.
The patient
A 58-year-old man presented to the hospital with worsening of shortness of breath associated with known COVID-19 infection. He had been well until 10 days before admission when his shortness of breath began and he was diagnosed with COVID-19 pneumonia.
His past medical history included hypertension, hyperlipidaemia, prediabetes, obesity, and benign prostatic hyperplasia. Medication included alfuzosin 10 mg daily, amlodipine 10 mg daily, aspirin 81 mg daily, atorvastatin 40 mg daily, chlorthalidone 25 mg daily, and losartan 100 mg daily,
On examination, his temperature was 38.3 °C (101 °F), blood pressure 146/92 mmHg, heart rate 65 beats per minute, respiratory rate 20 breaths per minute, and oxygen saturation 97% on room air. Pitting oedema (swelling) was noted in the both lower legs.
His blood tests at presentation showed a sodium of 136 mmol/L, potassium 3.4 mmol/L, urea 44 mg/dL, creatinine 2.6 mg/dL (230 mcmol/L, indicative of acute kidney injury), calcium 8.1 mg/dL, and albumin 3.2 g/dL
Management focused on acute hypoxic respiratory failure, and the patient was treated with supplemental oxygen, remdesivir, and dexamethasone.
His hospitalisation was complicated by further worsening of his acute kidney injury with the blood creatinine rising to 5.2 mg/dL (460 mcmol/L) over a 7-day period. For the first 12 weeks, the patient took 60 mg of prednisone daily. The patient then had a kidney biopsy.

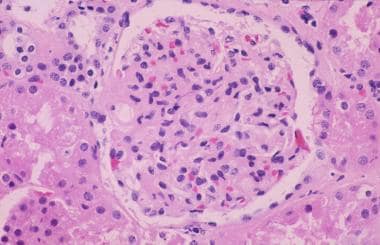
The patient’s kidney biopsy, with a glomerulus showing collapsing FSGS.
After that period, 24-hour urine collection was repeated and showed an almost 10-fold reduction in proteinuria. In addition, serum creatinine had improved to 3.2 mg/dL (283 mcmo/L). A slowly tapering course of prednisone was completed over the following weeks. At 22 months, the creatinine was 2.6 mg/dL (230 mcmol/L) and stable.
In conclusion, the authors presented a case of COVAN which was successfully treated with steroids, and at 22-month follow-up patient remained in full remission
Other resources
These are two review articles about COVAN: Velez, 2020 and Kim, 2023
And CKDEx has more information on HIVAN.
Last Reviewed on 26 June 2024