Progression of CKD and when doctors get concerned
Stage 4 CKD (with a GFR under 30 ml/min) – is when doctors get concerned about CKD. But it is not as simple as that (see later) [“is it ever?!” CKDEx Ed].
Let’s go through the 5 stages, and discuss more about when they get concerned.
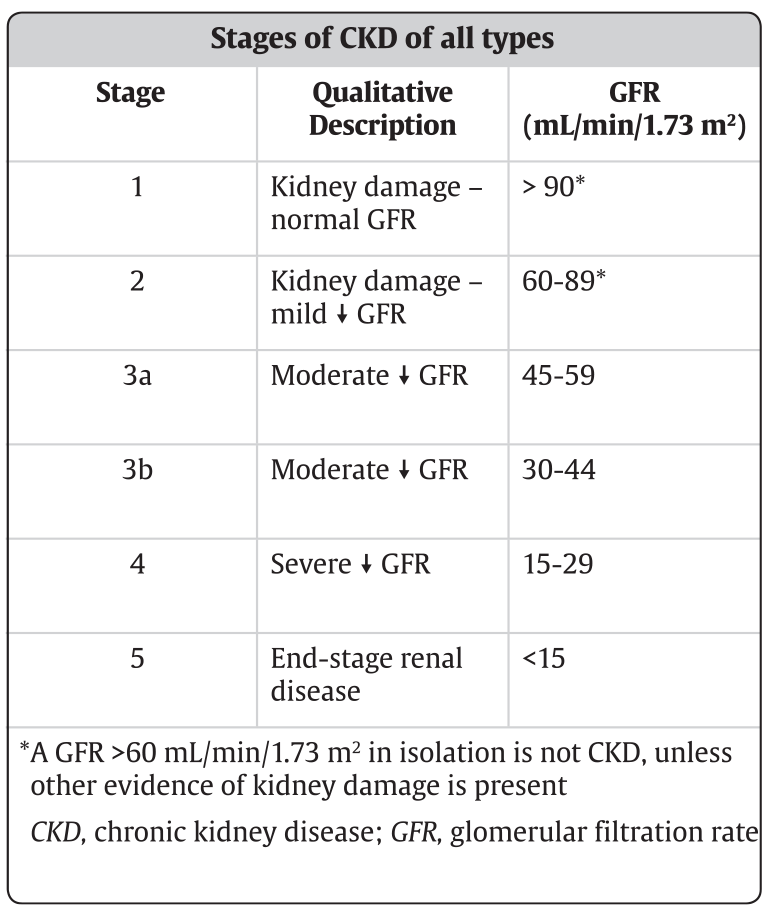
CKD Stages
These are the 5 stages (with stage 3 split into two) in the CKD classification, which are based on something called estimated GFR (eGFR) (normal is 90-120 mls/min).
eGFR is a blood test which estimates the level of function of the kidney. GFR is in turn is based on the blood creatinine level. The lower creatinine and CKD stage, and higher the GFR, the better.
‘Progression of CKD’
CKD does not always progress. Thinking that is does, is a common false belief. But for some patients, it does slowly ‘progress’ – i.e. worsen, from a very mild problem (CKD1-2) to kidney failure (CKD5) that is life-threatening.
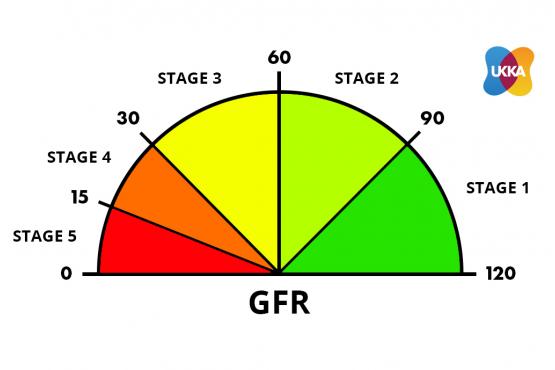
Courtesy of UKKA
CKD Stage 1+2 – Kidney damage or structural kidney problem (with normal kidney function) (eGFR 60-120 mls/min)
- Symptoms: no symptoms
- Doctors concern: little. There is no specific treatment needed for this stage of CKD. Risk factors for CKD should be looked at and treated if needed (for example high blood pressure).
CKD3A – Early mild CKD (eGFR 45-60 mls/min)
- Symptoms: no symptoms (usually)
- Doctors concern: mild. Doctors will focus on treating the cause of CKD and making sure blood pressure and blood sugars are in the correct range (if diabetic). This will help stop CKD worsening.
CKD3B – Later mild CKD (eGFR 30-45 mls/min)
- Symptoms: no or mild symptoms
- Doctors concern: some. Doctors will focus on treating the cause of CKD and making sure blood pressure and blood sugars are in the correct range (if diabetic). This will help stop CKD worsening
- GP (primary care): should discuss you with a nephrologist (specialist kidney doctor).
Note 1. CKD3B is worse than CKD3A
Note 2. CKD symptoms (described here) usually start if patients move from CKD3B to CKD4.
CKD4 – Moderate CKD (eGFR 15-29 mls/min)
- Symptoms: moderate
- Doctors concern: significant. A nephrologist should find the cause and treat your CKD, ensuring blood pressure and blood sugars are in the right range.
- GP (primary care): should refer you to a nephrologist (and you be seen in 4-6 weeks ideally, faster if deteriorating rapidly). The nephrologist will now usually start taking the lead in your care. Specific treatments for your cause of CKD may also be required.
Note. CKD4 means you may require dialysis or a kidney transplant one day.
CKD5 – Severe CKD (kidney failure) (eGFR < 15 mls/min)
- Symptoms: severe
- Doctors concern: high. Nephrologist should now lead, and be starting dialysis and/or preparing you for a kidney transplant, or giving supportive care (i.e no dialysis/transplant)
- GP: should stay in communication with nephrologist, and deal with non-kidney problems.
Note. CKD5 means you require dialysis, or a kidney transplant, or supportive care (no dialysis).
At what stage of CKD should you see a nephrologist?
CKD Stage 4. That is the short answer.
You should see a nephrologist, when your eGFR is less than 30 mls/min. This occurs at Stage 4 CKD.
The creatinine blood test is likely to be 150-200 mcmol/L at this point (normal is 60-120 mcmol/L; or 0.6-1.2 mg/dl in USA).
Outlook for CKD
Overall the outlook is good. Even though CKD is common (10% of the population), only 1 in 100 develop kidney failure (CKD5) and need dialysis or a kidney transplant.
- CKD stages 1-5 are very different, with different outlooks; generally the higher the level of CKD, the worse the outlook
- CKD does not always progress, e.g. CKD1 to 2, CKD2 to 3 etc
- CKD is associated with other long-term diseases that affect longevity, e.g. diabetes, ischaemic heart disease (IHD), and high blood pressure. So CKD patients often has these problems too. This makes it hard to determine what is affecting the outlook for patients with CKD
- Some people with CKD get better, with no evidence of CKD.
Importance of age and rate of decline
It is not just about the level of kidney function (and stage). The age of the patient and rate of decline are often more important than the number.
For example, a 29 year old with CKD1 (creatinine 64 mcmol/L, i.e. normal) that progresses to CKD3B (creatinine say 108, high-normal) in 6 months, is of more concern to a doctor than and 89 year old with stable CKD4 (creatinine 254).
The latter is likely to die with the problem, not of it. The former may need dialysis (or a kidney transplant) 5 years later, which has a major effect on longevity (how long they may live for).
Diagram below is not true
As it implies there is a natural ‘progression’ (worsening) from left to right. This does not usually happen.
Does CKD get better?
Yes, it can do. In fact, in this large Canadian study, advancing age, CKD regression (getting better) or death (i.e. die with it, not from it) were more likely than CKD progression or kidney failure: Liu, 2021.
Summary
We have described the progression of CKD and when doctors get concerned. Not all patients progress. The patient’s age and rate of decline of GFR are important. We hope it has been helpful.
Other resource
At what stage should you see a nephrologist?
Last Reviewed on 24 June 2024