What do you need to know about chronic kidney disease (CKD)?
Keep track of your kidney data with PKB
Key points
- Where are the kidneys? Near the middle of your lower back, on either side of spine
- What do the kidneys do? Body’s dustmen
- What is CKD (chronic kidney disease)? – long term reduction in kidney function OR abnormal kidney structure (with normal function). A mild form is very common – affecting up to 10% of the population. For many of these, CKD is really a risk factor for a more serious problem later in life. This can be addressed which is why only 1 in 100 people end up requiring dialysis or a kidney transplant
- How is CKD diagnosed? CKD stage/eGFR classification
- Causes of CKD – 7 groups – unknown (with small kidneys) and diabetes are the commonest
- Symptoms of CKD – shortness of breath and ankle swelling are red flag symptoms
- What treatment can the doctor offer? Even though CKD is not normally curable, there is alot doctors and the NHS can do. Does everyone with CKD need treatment? No
- What can I do to help myself? There are THREE important things you should do. See below
- How often do I need my eGFR/creatinine measured? – very variable
- What is the outlook for CKD? – generally good, but very variable.
So. What do you need to know about CKD?
1. What is CKD (chronic kidney disease)?
Chronic Kidney Disease (CKD) means a long term reduction in kidney function, or a structural problem with the kidneys (with normal function). It affects both kidneys, and usually comes on over months or years.
The words ‘chronic’ and ‘acute’ mean long and short term. Neither word implies ‘good’ or ‘bad’. Male pattern baldness is a ‘chronic’ normal variant and not a disease. A sore throat that gets better in 2 days is an ‘acute’ illness.
CKD may result in failure to maintain the balance of water and chemicals (including acid) in the body. This is because the normal function of the kidneys is to be the body’s dustmen, and keep the levels of chemicals and water stable.
2. How is CKD diagnosed? CKD stage/eGFR classification
It is surprisingly easy to diagnose, define and classify. It requires more than a doctor taking a history (asking questions) and examining you – but that should happen as well. After that, you will need these 3 big tests:
- Blood tests – mainly eGFR and creatinine (on which GFR is based) – higher the GFR, lower the creatinine the better
- Urine protein level – as indicated by the urine ACR, uACR) – the lower the uACR the better
- Kidney ultrasound scan (in many). It should show two normal kidneys >10cm in length.
After that, CKD is classified according to its severity, based on the called eGFR (estimated glomerular filtration rate) – the higher the eGFR, the better the function. Normal eGFR in humans is 90-120 mls/min.
The eGFR is based on a simple blood test called creatinine (normal range 60-120 mcmol/L); the lower the creatinine, the higher is the GFR, the better.
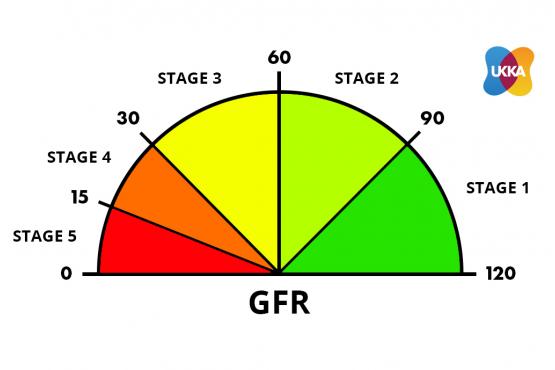
Courtesy of UKKA
What is the 5 stage CKD/eGFR classification?
Normal human GFR is 90-120 ml/min.
CKD1+2 – risk factors for CKD (eGFR 60-120 ml/min)
CKD3A – mild CKD (eGFR 45-59 ml/min)
CKD3B – mild-moderate CKD (eGFR 30-44 ml/min)
CKD4 – moderate CKD (eGFR 15-29 ml/min)
CKD5 – severe CKD (kidney failure) (eGFR < 15 ml/min)
– CKD4 means you may require dialysis or a kidney transplant one day
– CKD5 means you will require dialysis, or a kidney transplant, or supportive care (no dialysis).
Note. CKD is different from Acute Kidney Injury (AKI), which is rapid onset kidney failure with different causes and treatments. This comes on over hours or days. It is not the focus of this article.
3. How common is CKD, and why is it important?
A mild form is very common, affecting up to 10% of the population – making it one of the most common chronic diseases. Fortunately only 1 in 100 people go to develop kidney failure (CKD5) and require dialysis or a kidney transplant – i.e. about 1 in 1000 of the population are on dialysis or have a kidney transplant.
It is also linked to other very common diseases: high blood pressure (BP; also called hypertension), diabetes and chronic heart failure (CHF).
2-5% of the population have diabetes, which is the most common known cause of CKD.
Who is at risk of CKD?
Anyone can get it. But these are the main risk factors:
- Age – more common as you get older
- Gender – more common in men
- Ethnicity – Black and Asian people are at higher risk
- Smoking
- Family history
- Previous acute kidney injury (AKI) episode(s).
The most common age at which dialysis is started is 60-65 years.
Anyway, why is CKD important?
There are two reasons. Firstly, the dustman role is important. In other words toxins and water build up in the body if they are not removed by the kidneys. And secondly, a small number of people go on to needing kidney dialysis or a transplant.
4. Does everyone with CKD need treatment?
No. CKD is a spectrum, ranging from mild damage (CKD1-3) to advanced disease (CKD4-5) where the kidneys fail to work. Most patients have milder forms and will be able to control their CKD with lifestyle changes and regular medication review by their GP or practice nurse.
However, 1 in 100 patients will experience worsening of their CKD despite these measures, and may ultimately require dialysis (haemodialysis or peritoneal dialysis) or a kidney transplant.
5. What are the causes of CKD?
There are 7 groups of causes:
- Unknown (often with small kidneys). This is the ‘cause’ in 30% of patients
- Diabetes (mainly type 2). This is the cause in 20% of patients, i.e. the second commonest
- Renovascular disease. This mainly occurs in older people who are smokers or ex-smokers; and/or people with congestive heart failure. It is then called ‘cardiorenal syndrome’
- Obstructive nephropathy. This means a blockage in the drainage system of the kidneys – i.e. ureters, bladder, or prostate (in men). It is usually due to prostatic disease in a men, or cancer in the pelvis in women. Kidney stones can cause it, but are not a common cause (unless you have one kidney)
- Glomerulonephritis / vasculitis. These are ‘autoimmune’ (of which there are 7 types). This means the body’s immune system (normally its defender) attacks the small blood vessels within the kidneys
- Tubulointerstitial disease. ‘Tubulointerstitial disease’ is not really just one diagnosis. The phrase refers to a group of kidney conditions that mostly affect the tubules. Tubules are structures largely in the inner area of the kidney (medulla) responsible for processing urine. The tubules are shown in the diagram below. Each glomerulus has a tubule and together they are called a ‘nephron’. There are three groups of causes include: autoimmune, drugs and infection (e.g. reflux nephropathy). The drug causes include non-steroidal anti-inflammatory drugs (NSAIDs; if they are used long-term, especially at high doses), lithium, ciclosporin and tacrolimus
- Polycystic kidney disease. This is an inherited condition where multiple cysts form on the kidney. It is the only common familial (inherited) cause.
Notes. Simple primary (essential) high blood pressure and simple recurrent urinary tract infections (UTIs) do not cause CKD. A doctor should find another cause in such a patient with simple high BP or UTIs.
The causes of CKD in children and young adults are different.
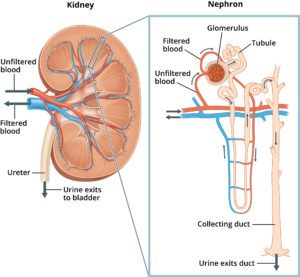
Diagram above shows the tubules and kidneys.
6. What are the symptoms of CKD?
- Swollen ankles, feet, hands or face (especially around the eyes) – as a result of water retention (oedema). Ankle swelling is a red flag symptom in CKD, and should never be ignored
- Shortness of breath – also a result of water retention. Shortness of breath is also a red flag symptom in CKD, and should never be ignored
- Tiredness
- Frothy urine and an increased need to pee – particularly at night
- Itching
- Pain
- Difficulty sleeping (insomnia) and concentrating
- Weight loss (or gain) and poor appetite.
Note. There may be no symptoms, especially in milder forms, e.g. CKD1-3. These stages of CKD may be picked up by a routine blood test. In this way it is initially a ‘silent disease’ – like high BP, cholesterol and early diabetes. Hence simply taking a medical history to make (or exclude) the diagnosis is not enough. You need blood tests.
Also many of these symptoms are non-specific, and can be seen in other conditions, like heart failure. The symptoms of CKD in males and females are largely the same. The causes of many CKD symptoms are not fully understood.
7. What can I do to help myself?
There are the THREE important things you can do to help yourself.
1. Monitor (and write down) the 2-3 numbers written below. The blood and urine tests can be performed and monitored by your GP, but you can do a lot of this yourself; to help GP and nephrologist (hospital kidney specialist) if you have one.
- Creatinine blood test. This is the most reliable measure of kidney function; the higher the number the worse the kidney function. It should be below 120 mcmol/L, and be measured every 3-6 months – more frequently if CKD worsens
- eGFR. The creatinine level determines your eGFR and hence CKD stage – the higher the creatinine, and lower eGFR, the higher (i.e. worse) CKD stage [“yes it is confusing” Ed]. eGFR should be above 60 mls/min, ideally above 90 mls/min. It should be also measured every 3-6 months
Note. You can chase your own blood tests using the Patient Knows Best (PKB) website - Protein in the urine. Some patients need urine protein measurements too, this is calculated with a simple urine test. When the kidneys leak protein it is a sign of strain. It is called a ‘uACR’ (urinary albumin-to-creatinine ratio). Again, you should chase the protein level – again via Patient Knows Best.
2. Blood pressure – make this a primary focus. Having normal or low blood pressure is the most useful thing you can do for CKD. So, buy a BP machine from any chemist or large supermarket or Amazon – prices vary, approximately £20-£40. ‘A&D’ is a good make. Take your own BP once a week until stable.

Get your BP checked. Better still buy your own machine and check it yourself.
3. Know your medication. Many people with CKD take alot of medication: to lower blood pressure (especially two types of blood pressure medicine, ACE inhibitors and ARBs); remove fluid (diuretic, i.e. water tablet), control blood glucose, and lower cholesterol. In more advanced CKD they may take vitamin D, a phosphate binder and erythropoietin (EPO). It is important to understand your medications, and take them as prescribed. Do not run out.
Is there anything more I can do?
Yes.
- Lose weight (if you are overweight). For many patients with CKD, being overweight or obese is a major factor – as it causes diabetes and high BP. So, if requested by a doctor or nurse, please start to lose weight and it will help a lot
- Blood pressure (BP) tablets. Most patients with CKD have high BP. The treatment of high BP is more effective if you follow a low salt diet (see below). Talk to a dietitian or GP about that. Here is more information on how to lower BP
- Angiotensin-converting enzyme inhibitor (‘ACE inhibitor’; e.g. Ramipril) or angiotensin II receptor blocker (‘ARB’, e.g. Losartan). Two types of blood pressure tablets, ACE inhibitors and ARBs, may slow CKD and delay kidney failure, even in people who don’t have high blood pressure. The names of these medicines end in ‘–pril’ or ‘-sartan’. This is because they have a special effect on the kidneys as they reduce protein levels in the urine, which is damaging. Ask your GP to be considered for one, if you are not taking one already
- Sodium-glucose cotransporter 2 (SGLT2) inhibitor (e.g. Dapagliflozin) – are a newish class of diabetic tablets that reduce blood glucose levels by increasing urinary glucose excretion. They also may slow CKD and delay kidney failure. And they have also been shown to be useful for many patients with diabetes (especially DM2) and heart failure (CHF) – especially if there is a lot of protein in your urine (with or without diabetes). Again, ask your GP if you are not on one.
- Specific treatments – for different diseases exist. Make sure those specific treatments have been considered, and started if appropriate
- Diet. There is no such thing as a ‘CKD diet’. In the earlier stages it is OK to eat normally. Later on dietary restrictions or encouragements may be advised. A low salt and protein diet may help to control CKD symptoms. You can request to be referred to a dietitian
- Support network. It is important to build up a support network of friends, family members, healthcare professionals, organisations, charities and patient groups that you can go to for help, advice and information – if you need it.
8. Are there any extra things you can do if you have bad CKD (CKD4-5)
Yes. 3 big things.
- Erythropoeitin (EPO). Many patients with CKD4-5 have anaemia (lack of blood in the body) as the kidney makes a substance called EPO that stimulates the bone marrow to make red blood cells. As CKD advances, less EPO is made and anaemia develops. This is easy to treat with an injection once a week (e.g. darbepoetin alfa) or a tablet 3 times a week (e.g. roxadustat) and will give you more energy. Ask your doctor or specialist nurse
- Transplant referral. Most CKD4-5 patients assume that if they are being prepared for dialysis, they are going to be put on the transplant waiting list. Assume nothing. Check check check. You are only on the waiting list when you are written to, and the letter says you are on it
- Ask your loved ones to be kidney donor. Again, if you are in the CKD4-5 group, a loved one (partner, friend or relative) may be able to give you a kidney. Ask them. This is best done in a quiet one-to-one chat.
9. What else can the NHS do?
- GP Practice Nurse. Many GPs have a practice nurse that runs a ‘long-term condition’ clinic; including chronic kidney disease, on their own. Ask for three monthly reviews there. Some of them work with a clinical pharmacist who can do a similar role.
- Hospital specialist kidney doctor. These are called a nephrologist or renal physician or doctor. If you have CKD4 or CKD5, your GP should refer you to one of them. They will be senior, either a consultant (boss) or their deputy called a registrar. They work at a hospital kidney (renal) unit. You may need to travel to a bigger ‘teaching’ hospital, as smaller local hospitals often do not have them. People with CKD1, 2 and 3A will not need a referral.
- As the patient ..
Ask for review and monitoring of creatinine/eGFR every 3-6 months, more frequently if CKD worsens – this can be virtual, (blood tests reviewed from afar). They can also get you to see a CKD specialist nurse and/or refer you to a dietitian.
When you see a consultant, only let them discharge you when your kidney condition is stable. If you are discharged, make sure you have the phone number (and email address) of the consultant’s secretary. So, if you need to be seen again (say if kidney function is worse, or you are worried), you can arrange a (re) referral rapidly.
Note. If referred to a hospital kidney doctor by your GP, you will be seen well within 18 weeks, a key NHS target. If your GP wants you seen any sooner, they will need to email (or ring) a kidney doctor. If you are worried, you can ask them to do that.
10. What is the outlook for CKD?
This is not easy to answer. Why?
- CKD stages 1-5 are very different, with different outlooks; generally the higher the level of CKD, the worse the outlook.
- CKD does not always progress, e.g. CKD1 to 2, or CKD2 to 3 etc.
- CKD is associated with other long-term diseases that affect life expectancy, e.g. diabetes, ischaemic heart disease (IHD), and high blood pressure. So CKD patients often have these problems too. This makes it hard to determine what is causing the outlook for patients with CKD compared to similar aged patients. To do this, complex maths is required.
The Kidney Failure Risk Equation (KFRE) can be used to predict your risk of the need for dialysis and transplant (CKD5).
Summary
We have described what do you need to know about CKD. We hope it has been helpful.
[“Yes, it is confusing. There are so many terms that relate to kidney disease – e.g. renal, renal physician, nephrology, nephrologist, transplant, dialysis, CKD, AKI etc. Wish they would make their minds up” CKDEx Ed].
Top Tip
If you are referred to a nephrologist (kidney specialist) make sure you have a kidney ultrasound. It often shows information that will help you.
Other resources
CKD: your questions answered (shorter version of this article)
10 IHD facts
10 CHF facts
10 diabetes facts
10 cholesterol facts
Last Reviewed on 22 June 2024