What is HIVAN (HIV-associated nephropathy)?
History
AIDS was first reported in 1981.The first reported cases of HIV-associated nephropathy (HIVAN) were described in 1984. Thus it was described early in the HIV epidemic in the USA, especially in urban centers serving large numbers of HIV-positive people of African descent. In the early 1990’s, HIVAN was the most rapidly increasing cause of ESRD in the USA.
Let’s learn more about HIV-associated nephropathy (HIVAN).
Who gets HIVAN and how does it present?
HIVAN is primarily associated with HIV subtype 1, especially in individuals of African descent. Patients usually present with rapidly progressive chronic kidney disease (CKD), associated with severe proteinuria (protein in the urine), and advanced HIV disease/AIDS (with of CD4 counts <200 cells/mm3). But there is no one blood test that accurately predict which patients will get HIVAN.

Patients typically have enlarged bright kidneys on kidney ultrasound, as above.
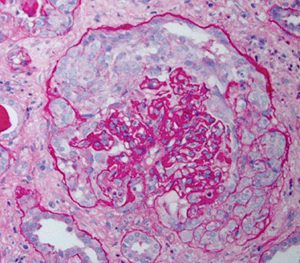
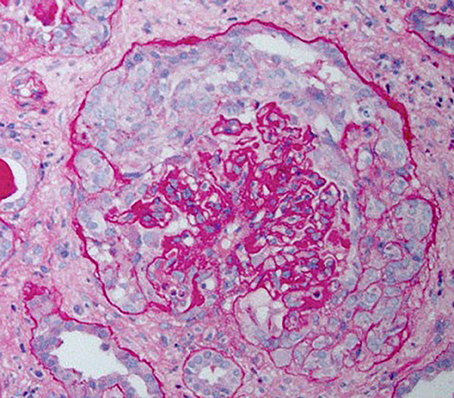
Kidney biopsy showing a glomerulus, which shows a typical collapsing form of focal and segmental glomerulosclerosis (FSGS).
This classic presentation is rarely encountered in patients receiving combined antiretroviral therapy (cART).
Treatment of HIVAN
Combined antiretroviral therapy (cART) is the cornerstone of management of HIVAN – and steroids may be added on a case-by-case basis.
Effective control of HIV replication can slow the progression of kidney disease. Other management strategies include medication to control blood pressure, reduce proteinuria, and manage complications.
But the widespread use of combination antiretroviral therapy (cART), has resulted in a marked reduction in the likelihood of getting HIVAN in the first place.
And, if HIVAN does occur – being effectively treated by cART – there are much lower levels of proteinuria and slower progression to severe CKD/ESRD occurs. This reduces the likelihood of a kidney biopsy. So this is another reason rates of HIVAN have fallen significantly.
Diagnosis of HIVAN
Since HIV-positive patients are at increased risk for other comorbidities that also cause chronic kidney disease, including diabetes mellitus and hepatitis C infection, a kidney biopsy is required to definitively diagnose HIVAN.
HIVAN and kidney transplantation
Historically kidney transplantation was initially thought not to be possible in HIV patients, due to the fear of further immunosuppression from anti-rejection drugs.
But now kidney transplantation is increasing in HIV-positive patients with end-stage renal disease (ESRD). Although the rejection rate is high, the kidney survival rates are high. Successful kidney transplantation from HIV-positive donors to HIV-positive recipients has been reported as well.
Prognosis (outlook) for HIVAN
Historically, HIVAN led to rapidly progressive ESRD. However, in the modern era, combination antiretroviral therapy (cART) has significantly improved the prognosis of HIVAN.
HIVAN and COVAN (COVID-19-associated nephropathy)
In recent years, the attention of research has shifted from HIVAN to COVID-19-associated nephropathy (COVAN). Like HIV-1, SARS-CoV-2 coronavirus affects interferon, and hence COVAN shares the same collapsing features as HIVAN.
Summary
We have described what is HIVAN (HIV-associated nephropathy). We hope it has been useful.
Other resources
This is a typical case of HIVAN: Tan, 2023.
Here are three review articles on HIVAN: Rednor, 2018, Rivera, 2022 and Rivera, 2023
And this is a review of COVAN: Velez, 2020.
Last Reviewed on 22 November 2023