What is reflux nephropathy?
Reflux nephropathy (RN), is also known as vesicoureteral reflux (VUR) or just ‘reflux’. Reflux nephropathy was previously called chronic pyelonephritis
But what is it? Reflux is either a congenital (i.e. you are born with it): or acquired condition – where urine flows backward from the bladder into the kidneys, potentially causing CKD (in a minority) over time. The underlying cause(s) is not known.

The primary cause of reflux nephropathy is a defect in the valve-like mechanism that normally prevents urine from flowing back into the ureters.
Here are 10 facts about reflux nephropathy,
1. Definition
Reflux nephropathy is a disorder where urine, instead of flowing in a unidirectional manner from the kidneys to the bladder, flows backward from the bladder to the kidneys. It may affect one or both kidneys.
2. Who gets it?
It is a relatively common condition (1-3% of children) and is usually asymptomatic. The diagnosis is often missed in early childhood as it presents in early adulthood and women of childbearing age.
It is more common in women, and is partially inherited especially from mother to daughter.
Reflux nephropathy is the second most common cause of chronic tubulointerstitial disease (TID) and the fourth common cause of ESRF in children (10-15%).
3. Congenital or acquired?
Both. In children, RN can be acquired or congenital. Acquired RN is more common among female children and is diagnosed mostly after a febrile UTI. A young child with a UTI should be assumed to have RN or some other other structural defect of one/both kidneys, and be fully investigated by a paediatric nephrologist (hospital kidney specialist).
Whereas, congenital RN is usually diagnosed antenatally by ultrasound (whilst the baby is inside their mother) or during early follow-up, with no prior UTI, and is more common in male children.
In pregnant females with RN, approximately 40% of the offspring will have the condition, and testing of offspring is highly recommended.
4. Urinary tract infections
Individuals with reflux nephropathy are at an increased risk of urinary tract infections (UTIs) because bacteria can more easily travel from the bladder to the kidneys.
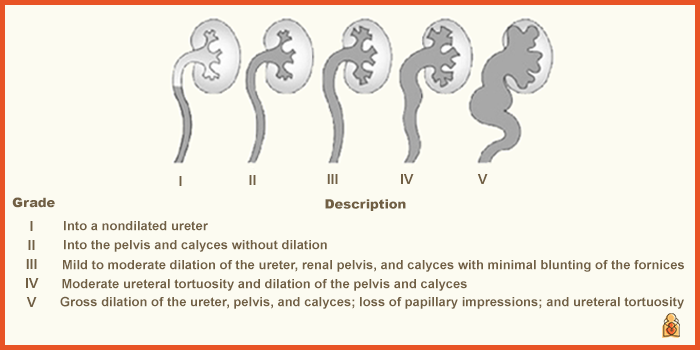
5. Grading system
Reflux nephropathy is graded on a scale from I to V, with Grade I being the mildest and Grade V being the most severe. The grading system helps determine the extent of the reflux and its potential impact on the kidneys.
6. Symptoms
In many cases, reflux nephropathy is asymptomatic (i.e. no symptoms), especially in its early stages. However, recurrent urinary tract infections, high blood pressure, and CKD may eventually lead to symptoms.
7. Diagnosis
Tests such as kidney ultrasound (or CT or MRI) are used to make the diagnosis. They are also useful to assess the severity (grade) of the RN. Scars in the cortex may be seen. Nuclear medicine scans (including DMSA, DTPA or MAG-3) are useful both to confirm the diagnosis and to compare the proportion of effective urine coming from each kidney.
Association with scarring
The reflux of urine into the kidneys can lead to scarring of the renal tissue. Over time, it is this scarring that can affect kidney function.
Unilateral or bilateral scarring?
- 35% have unilateral renal scarring
- 25% have bilateral renal scarring.
In patients with bilateral renal scars, 85% have CKD with reduced estimated glomerular filtration rate (eGFR).
Micturating cystourethrogram (MCU)
Previously a more invasive (uncomfortable) x-ray called a micturating cystourethrogram (MCU) was done.
‘Micturating’ is a medical term which means passing urine. Cystogram means picture of the bladder. A catheter is passed into the bladder and x-ray contrast injected into the bladder. Pictures are taken while urine is being passed.
This gives the best pictures of reflux and can assess the need for surgery. But it is not pleasant, and carries a small risk of causing urine infection. In children, a micturating cystogram may need to be carried out using a short anaesthetic to put the child to sleep.
8. Treatment
Treatment may include long-term antibiotics to prevent or treat urinary tract infections. And in some cases, surgical intervention to correct the reflux, or to remove one of the kidneys. These operations are now unusual. The choice of treatment depends on the severity of the condition.
Early diagnosis and appropriate management of reflux nephropathy are important for preserving renal function.
9. Complications
- Growth retardation is observed from recurrent cystitis and pyelonephritis in affected babies
- Increased maternal complications (UTIs, hypertension, worsening of renal function)
- Rapid onset of accelerated hypertension during pregnancy
- Patients with more severe RN can develop hypertension (10%), proteinuria (25%), urine concentration defects, hyperkalemia, acidosis (type 1 renal tubular acidosis), and chronic kidney disease (CKD).
10. Outlook
With early detection and appropriate management, many people with reflux nephropathy can lead normal, healthy lives. However, in severe cases, complications as outlined above can occur. Some patients with CKD progress to kidney failure (Stage 5 CKD) and need dialysis and/or a transplant.
Summary
We have described what is reflux nephropathy. We hope it has been helpful.
Other resource
Review article: Aeddula, 2023
Last Reviewed on 9 June 2024