What is renovascular disease (RVD)?
This is a condition where there is narrowing or blockage of the renal (kidney) arteries, which supply blood to the kidneys. It leads to reduced blood flow to the kidneys, which in turn affects kidney function and raises blood pressure. It is also known as renal artery stenosis (RAS).
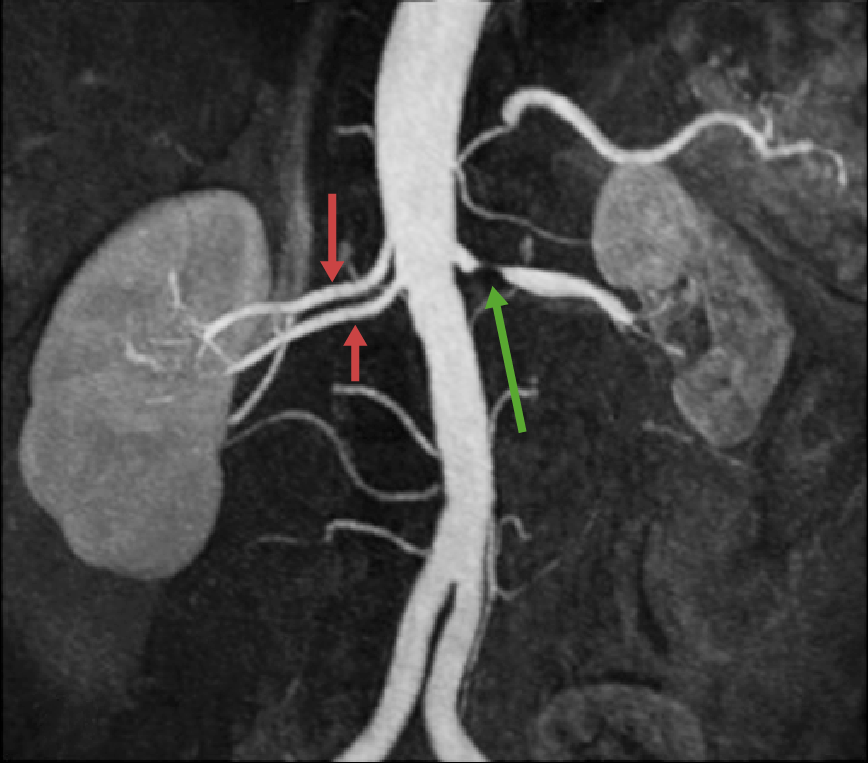
Typical renal (kidney) angiogram (x-ray) of (one-sided) RAS – showing a stenosis (tightening) of the left renal artery, and a (normal) ‘double artery’ to the right kidney. Such variants are common.
RVD is a common cause of chronic kidney disease (CKD) in older people, especially those who have smoked and/or have diabetes. Some patients progress to end-stage renal failure (ESRF) and require dialysis and/or a kidney transplant.
It can be unilateral (one-sided) or bilateral (both sides), usually the latter.
So. What is renovascular disease (RVD)?
1. Definition
RVD encompasses a range of conditions that cause narrowing or blockage of the renal arteries, which are responsible for carrying blood to the kidneys.
2. Causes
The most common cause of RVD (90%) is atherosclerosis (or atheroma), a build-up of fatty deposits (plaque) in the arteries. This is the same disease process that causes heart attacks and chronic heart failure (CHF, due to ischaemic heart disease, IHD), strokes and peripheral vascular disease (PVD). Patients with RVD often have (or have had) one of these problems as well.
When it occurs with heart failure (as it often does), the combination can be called ‘cardiorenal syndrome’, a name that implies that the underlying disease process (atheroma) is the same.
Patients with diabetes can have kidney problems due to two causes:
- Diabetic nephropathy – a diabetes-specific disease in which very small blood vessels in the kidneys are damaged, probably by the high sugar levels
- Renovascular disease – affecting the larger arteries.
Other rarer causes include fibromuscular dysplasia (FMD), a condition where the artery walls become thicker and less elastic. This especially affects young women and usually presents as very high blood pressure.
3. Hypertension (high blood pressure)
RVD usually leads to high blood pressure (hypertension) due to reduced blood flow to the kidneys. Bad hypertension is a key feature of RVD and can be the clue to the diagnosis – as it can be very difficult to control, requiring multiple high dose drugs.
The kidneys play a critical role in regulating blood pressure, and when their function is compromised, it usually leads to elevated blood pressure.
4. Renal ischaemia (lack of blood supply)
Reduced blood flow to the kidneys results in renal ischemia, a condition where the kidney tissues do not receive adequate oxygen and nutrients. This can lead to reduced kidney function and CKD. Some progress to ESRF and dialysis +/- a kidney transplant.
5. Symptoms
RVD often does not cause symptoms until it is advanced. This is a problem as it means that it often presents to hospital kidney specialist (nephrologist) too late – when less can be done to prevent dialysis/transplant.
When there are symptoms, these may include high blood pressure that’s difficult to control, unexplained CKD with a smaller kidney on one or both sides, or worsening of kidney function after starting certain blood pressure tablets (e.g. angiotensin-converting enzyme inhibitors (ACE inhibitors) or angiotensin receptor blockers (ARBs).
In a small number of patients, RVD can present as extremely high blood pressure and acute kidney injury (AKI, i.e. rapid onset kidney failure). This requires urgent care in hospital.
6. Diagnosis
For most patients with RVD it is a ‘clinical diagnosis’ i.e. made by a nephrologist based on a higher risk patient with a characteristic history/examination, and a characteristic pattern of kidney blood and urine tests, and kidney ultrasound. The ultrasound may show a smaller kidney on one or both sides (less than 10cm long). There are normal (or slightly raised) albumin (a form of protein) levels in the urine.
On examination there may be bruits (whooshing sounds) coming from arteries in the abdomen and upper thigh.

Sites of relevant bruits. The doctor should listen in all of these areas.
It is quite often a ‘diagnosis of exclusion’, i.e. the only cause left in an older person who has smoked, with a small or smaller kidney, or kidneys – when other diagnoses have been excluded.
If there diagnosis is suspected (but unclear), to diagnose RVD, other tests can be used including magnetic resonance angiography (MRA), computed tomography angiography (CTA), and renal angiography/plasty. These tests help visualise the blood vessels and identify any narrowing or blockages.
Unfortunately all three tests have significant risk of worsening kidney function that can lead to temporary or permanent dialysis (and death in a very small number of patients. This is why they are not often done.
7. Treatment
The treatment of RVD depends on its severity and underlying cause. In some cases, lifestyle modification (especially stopping smoking), and medication to control blood pressure and reduce cholesterol, is sufficient.
It is also important to stop drugs that may be making RVS worse, especially angiotensin-converting enzyme inhibitors (ACE inhibitors) or angiotensin receptor blockers (ARBs).
Diuretics (water tablets) may be required if the patient is fluid overloaded (shown by ankle swelling or shortness of breath, SOB).
A small number of patients will need to be prepared for dialysis (+/- transplant). The outlook on dialysis is not great, with patients surviving, on average, about two years from the start of dialysis.
A very small number of people require interventions like angioplasty and stenting to open up narrowed arteries.
Note. Most people with RVD do not need an angiogram/plasty/stent. This is partly as there is little evidence they are of benefit (see ASTRAL trial, 2009, STAR trial, 2009, CORAL trial, 2014 and review by Yesiltas, 2023).
CKDEx debates the pros and cons (mainly cons) of a renal angiogram/plasty in a blog.
8. Angioplasty and stenting
Angioplasty is a procedure where a catheter with a balloon is inserted into the narrowed artery and inflated to widen it. A stent (a small mesh tube) might be placed in the artery to keep it open and improve blood flow. This is rarely done.
9. Surgical bypass
In a very few cases where angioplasty and stenting are not possible, surgical bypass might be considered. This involves creating a new path for blood flow using a healthy blood vessel from another part of the body.
10. Prognosis
The prognosis for RVD depends on factors like the extent of artery blockage, the overall health of the patient, and the success of treatments. Early detection and intervention can improve outcome and prevent kidney damage.
It’s important to note that medical knowledge is constantly evolving, and early referral to a nephrologist is important.
Summary
We have described what is renovascular disease (RVD). We hope it has been helpful.
Other resources
Here is further information on RVD.
This is a review article by Bhokari, 2023.
There is more information on renal artery stenosis written by the renal team at UHCW Coventry.
Last Reviewed on 3 March 2024